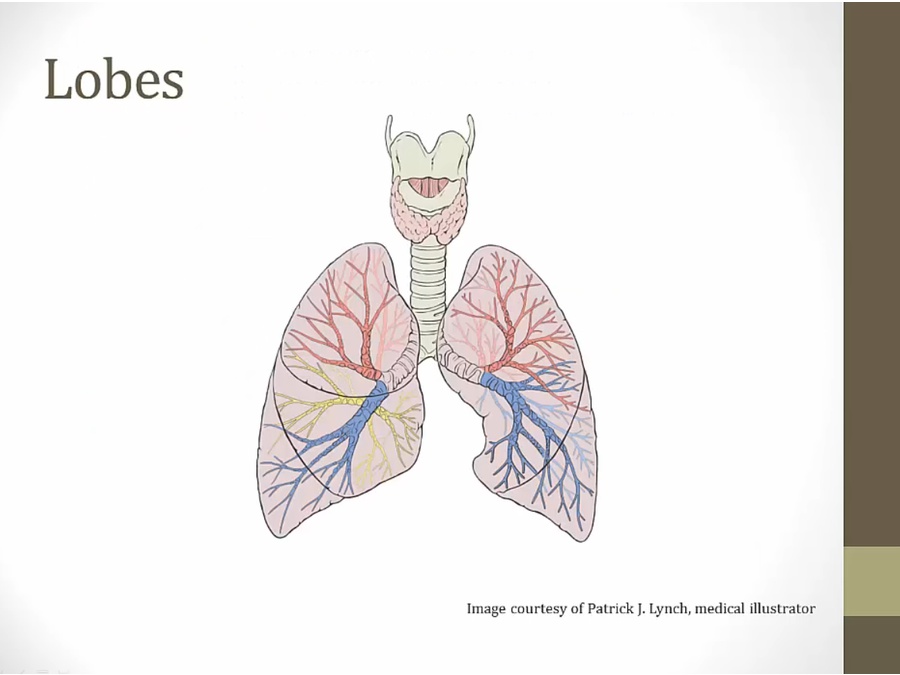
01 Pulmonary Anatomy
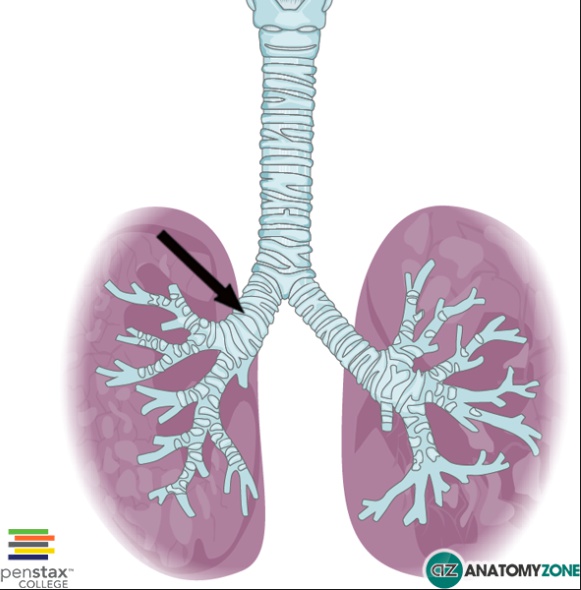
- left: sharp angle
- vomit and then pneumonia: usually right sided
- supine: superior portion of right inferior lobe or posterior portion of right upper lobe
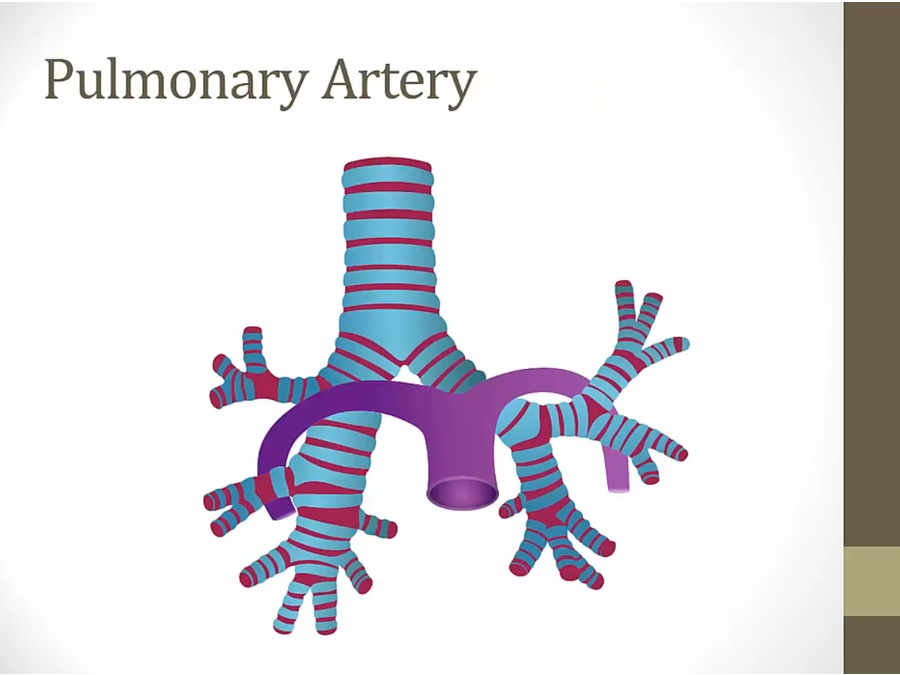
- right PA: anterior to right bronchus
- left PA: superior to left bronchus
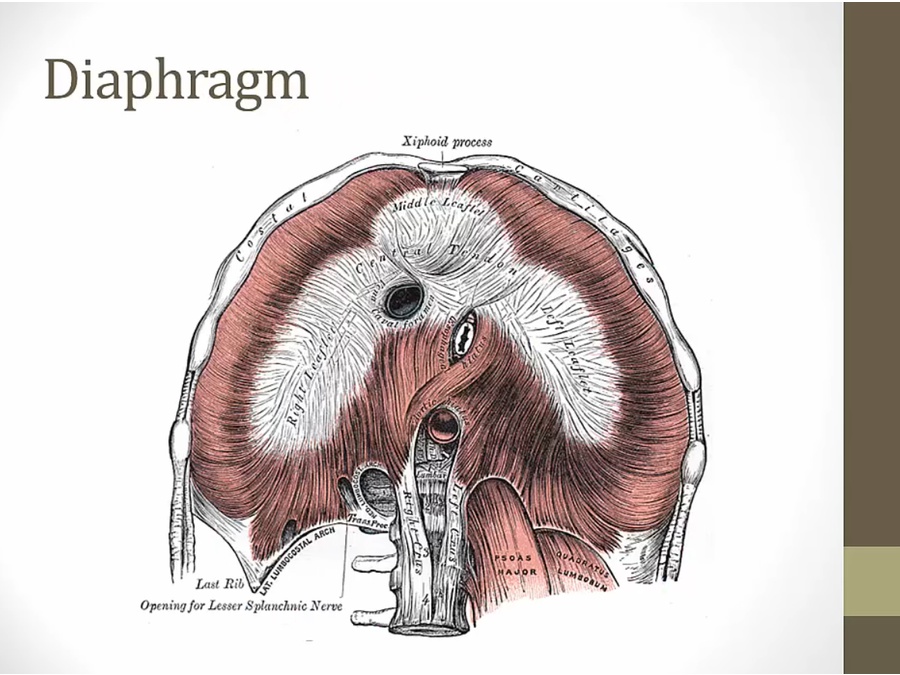
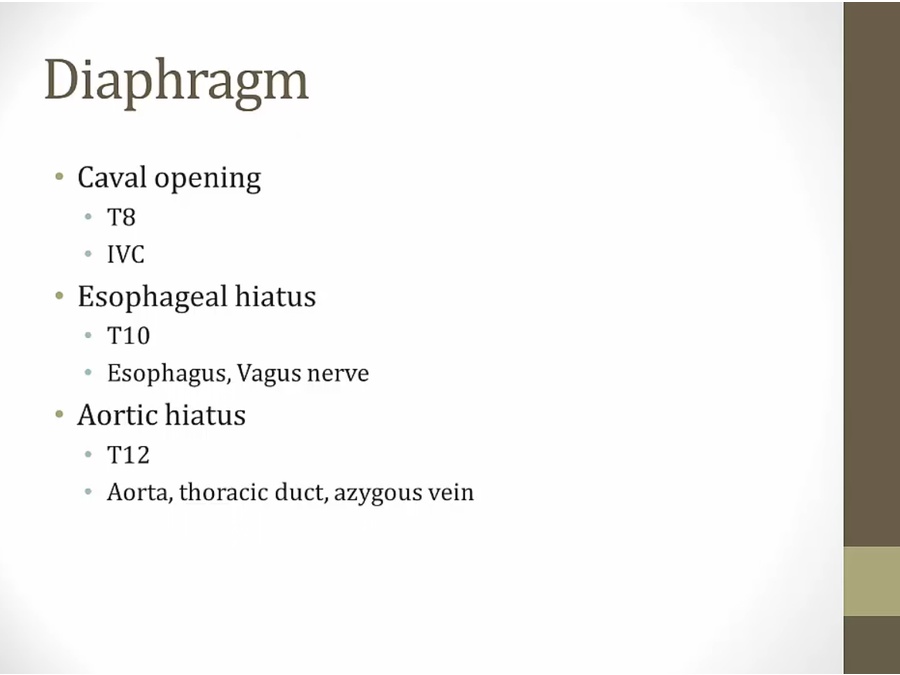
- caval foramen: IVC
- esophageal hiatus: esophagus
- aortic hiatus
- dyspnea: can't contract diaphragm to breath
- other side move down, push affected side up
Respiration
- quiet: diaphragm sole muscle
- accessory muscles: in hospital, see pts contract neck/abd when breathing = respiratory distress
Respiratory tract
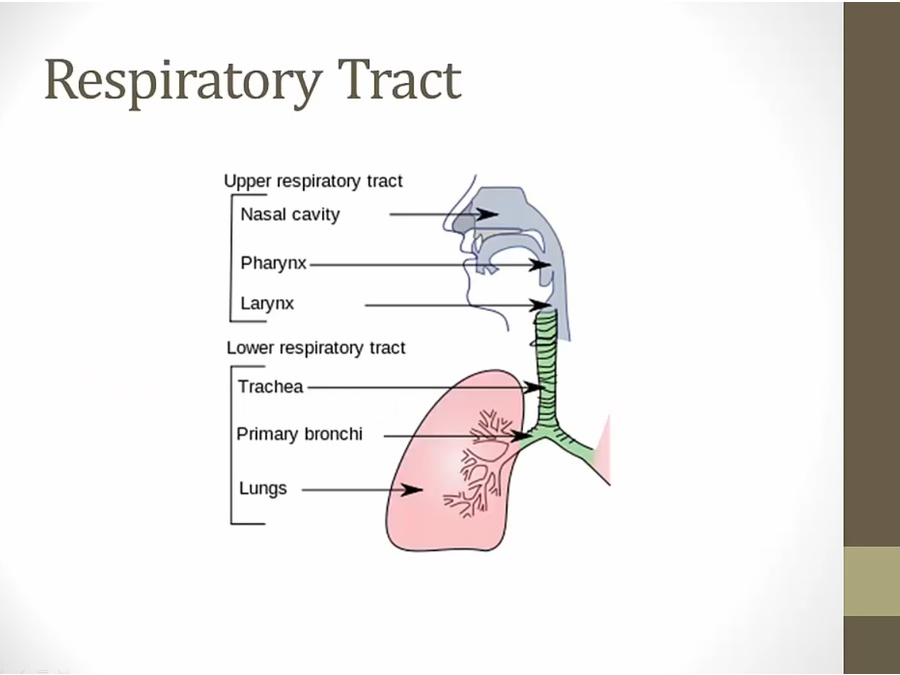
- URI: does not involve lower respiratory tract (sinusitis, pharyngitis, etc.)
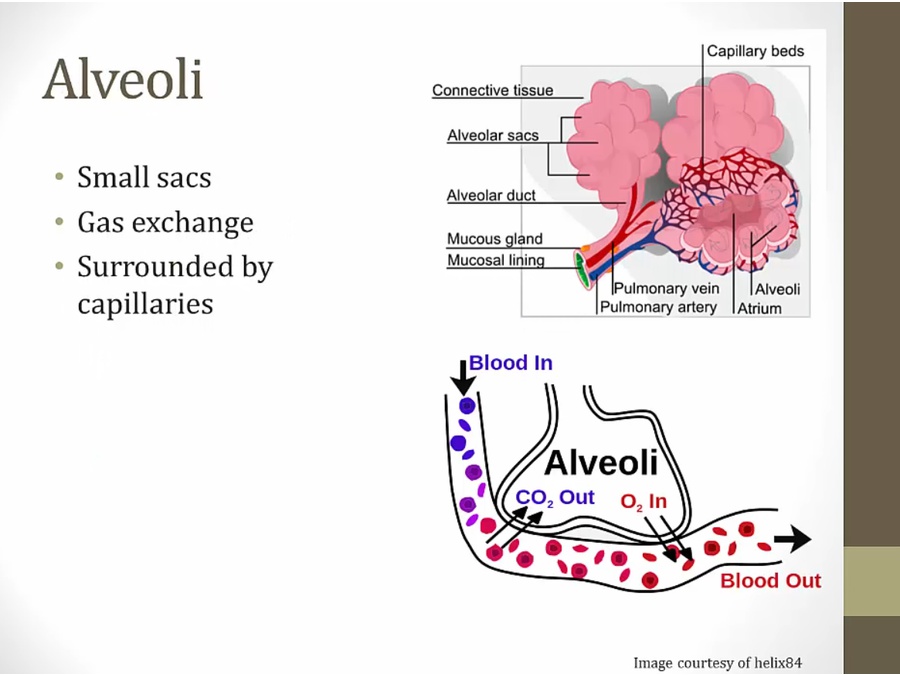
Alveoli
- clara: not in alveoli, in terminal bronchioles
Surfactant
- surfactant: alveoli stay open when exhale
- Laplace law
- if pressure in sphere below distending pressure, alveoli collapse
- low sphere: small radius, distending pressure high, takes more pressure to keep small sphere open, also more likely to collapse
- when inhale, alveoli gets large; when exhale, gets smaller
- result: when alveoli need the air to keep open, air leaves, distending pressure gets high
- surfactant shrinks surface tension as radius falls during exhalation
- when exhale, surfactant molecules gets closer, concentration higher, reduce surface tension
- falling radius and surface tension offsets one another
NRDS
- hyaline: glass like, what alveoli looks like
- give O2: all goes to healthy alveoli, sick ones collapsed (shunting)
- high glucose from mother stimulate baby's pancreas to make insulin
- all related to O2
- bronchopulmonary dysplasia: hyperplasia and fibrosis of airways (exposing premature lung to high O2 concentration, O2 toxicity)
Backlinks